In the final analysis, what is the value to CSD professionals of primary prevention activities? How can clinicians accommodate primary prevention fully into their clinical practices? What are the payoffs for making primary prevention a viable product line, within your speech-language pathology or audiology practice? How will your market share be affected by your new product lines? How will the professions evolve as a result?
For myself, I needed to answer some questions about how any new product line (in this case, primary prevention) can be successful, to determine if primary prevention can be a successful adjunct to evaluation and treatment. I needed to know:
* what exactly is this prevention product?
Education activities designed to help consumers lower, or avoid risks for communication and swallowing disorders
* can I easily explain this to other people?
We can help keep you well for expressing yourself, and to eat and drink.
* how can I make the abstract idea, a concrete entity?
Identify, assemble and present activities, selected to help consumers at risk maintain wellness.
* is anyone else doing this?
(Readers? You can help answer this. Thanks.)
* if so, what are the forces that make their products marketable?
High interest 1:1, small group and large group educational events, targeted to consumers' identified needs.
* what is my market area, my niche?
(Fill in the blank, readers)
* does my market area want this?
Observe the activity near you at fitness centers, weight loss nutrition programs, smoking cessation programs, farmers' markets, etc.
* how do I find out if my market area wants this?
Ask your consumers and friends on your digital social networks, if they are curious about how to stay well and avoid cardiovascular disease, cancer, diabetes, etc.
* how do I market this?
Use all communication channels that touch your desired market, and make it easy for consumers to reach you and HIRE you.
* what distinguishes me from other practitioners in this area?
CSD professionals can link their educational activities to clinical interventions, as consumers request services
* do I have the credentials for this work?
Speech - language pathologists and audiologists can pursue independent study and coursework in health promotion
* what will be successful outcomes of primary prevention work?
Consumers demonstrate increased knowledge in risk reduction strategies for communication and swallowing disorders
* HOW WILL I GET PAID?
Readers? Those activities not funded by grants and other external supports , might require a fee for service, to justify the time and costs incurred to teach consumers, who may never buy your clinical services.
Those of you who have a primary prevention product - how do you do it?
Trapping evil spirits....I like ice cream. I really do like ice cream. One story from our family lore that I frequently tell new consumers, is that I learned the actual value of a batch of ice cream - when I had to make it. Now that I regularly make batches of communication starter, the story seems as fresh as that hot summer day.
In the early 1960's, the ice cream technology available at my house was the wooden bucket fitted w/ hand crank. My Mom made it a very simple transaction for me: you help make it, you get to help eat it! The result of what seemed like three hours (I swear!) of hard relentless churning of that peach bit + creme anglais, was that we had fluffy - and slightly saline - peach ice cream for our hot summer party. I had churned away the evil spirits of lassitude, powered by the desire for a cool summer treat. My left arm also grew back, within two weeks.
Now, the joy of a thick, frozen bite of ice cream is dulled by political backlash directed at an ice cream company. This company leads its business model with its own social values; it has chosen to restrict its product to a country, whose policy is antithetical to these values. Refer to:
I like Israel. I really like Israel. One ice cream company is not bringing down the state of Israel. State governments in the US, who see themselves as the guardian of Israel's legitimacy within the country, have swung the battle - axe of politics down on this company. It's ludicrous, and almost pathetic that Israel supporters fear an ice cream company. Rather than freeze up Israel's management of its internal affairs, the company shared its moral vision to illuminate the moral shortcomings of the nation.
The political strike against the ice cream company embodies an act of zealotry. As the late Arkansas journalist Paul Greenberg put it, a zealot either agrees with you too strongly, or disagrees with you strongly.
Some writers, like Reza Aslan, say Jesus was a zealot. Other writers like Eric Hoffer might point to the example of an Obama voter, becoming a Trump voter in the next cycle, as the zealot's mark. Not strictly is the intensity of a person's devotion considered, but also how the focus on the devotion blinds the zealot to the full measure of that devotion. What could possibly be wrong with trying to punish Ben and Jerry's parent company, for B&J supporting a people they see as oppressed?
I really like people, like Bronowski, who have strong opinions. Whether they force me to work to eat, defend my favorite dessert, or justify a clinical judgement - I do enjoy the arguments. These days, I see a lot of zealotry, in the forms of inflexibility, in the field of CSD. It could be coming from the training a clinician receives in pre-service education, or through subsequent continuing education. It also can bleed through from some social - political movements that occupy your mind, but that are tangential to this CSD gig you've secured. It could even be as simple as letting the pressures of real life get in the way, by getting entrenched in clinical 'ruts', doing the same activities with persons carrying similar diagnoses. A clinician who participates in research studies, may surmise that the protocol is always the thing. Everything.
However you delineate the actions of persons on the train of a clinical/research movement; - when every case becomes a strict research protocol, without back - channel communication that can be crucial to the consumer moving towards her desired outcomes, it's zealotry. We are selling a service, albeit a professional service, and it seems sensible to deliver the service the consumer bought.
Zealotry = evil spirits? Only in the sense that your perceptions, your judgement can be clouded by adherence to a narrow frame of reference (dogma, allegiance to mentor/leader), that has political as well as scientific implications to your effective practice.
I really like the bottle tree. It reminds me of how important it is, to trap and stow away things that don't belong - things that can prevent you from safe passage on your clinical journey.
I recently started, after a break of almost twenty years, the mentoring of two new SLP professionals. Recently, I committed to consider a third - yikes! Mind you, I've mentored a few dozen new SLP's at all levels of their career development, since taking this career path: shadows of a clinician during the undergraduate years; interns in a medical setting, prior to their receiving the master's degree; and lecturing to graduate students about aspects of the 'hidden curriculum' - that is, what actually happens during the SLP's clinical workday.
The Clinical Fellow is approaching that very imposing finish line, in the marathon race to our professional credentials. Over the weeks, months and years of classroom study and clinical training, an SLP student in the classroom injects her didactic learning into clinical learning. With necessary clinical training in the University clinic setting and selected practica done, the intern then spends the better part of a term in a community's clinical setting, where theory first meets the workday road. Following that, the newly hired CF will show how independently they can apply their knowledge, to serve their consumers and the support systems.
And - the C's are only the MINIMUM qualifications for clinical practice. Training never ends!
When I first took on mentoring of young SLP's, the time interval overlaid that for the emergence for mitigation/prevention of serial harassment in the workplace. I had to deal with my perception of being a member of a significant minority in the field, who is also perceived by some as being a significant source of these problems in the workplace. It is what it is. It's a healthier and more productive workplace nowadays, and the forces of 'quid pro quo', 'hostile working environment' and appropriate workplace banter can go bidirectional. Anyone now completing their master's degree, and who has not yet internalized the lessons of serial harassment, will not make it as a CF. Parenthetical? It only shows that relating to your peers, is one lesson learned within the seminar called "Communication".
A CF remains psychically connected to her training program, and that's a good thing - because the idealism instilled by that discipline of class, clinic and practica, can easily carry over to her first paid workplace. The job of a mentor? Helping the CF sustain that idealism and enthusiasm, when her workplace tends to blunt or temper the role SLP may take in serving consumers. The CF is the local expert for her scope of practice, and makes her workplace more and more glad of that through the experience.
THIS BLOG POST, LIKE OTHERS IN THIS SERIES, DOES NOT ATTEMPT TO PROVIDE MEDICAL ADVICE. ALWAYS CONSULT A PHYSICIAN BEFORE MAKING SIGNIFICANT CHANGES TO YOUR HEALTH REGIMEN.
Primary prevention of cardiovascular disease; yep, we're still talking about that. Primary prevention interventions work to reduce or eliminate effects of the risk factors related to, in this instance, impaired function of the heart and blood vessels. Let's apply this basic premise to the recent trivia game this blog posted (1/17/21), about decisions you might make to manage risk to your cardiovascular system. We'll address each question in the game, citing the evidence currently available on each issue, then addressing what you might expect to come in the prevention movement. Here we go. The best answer for each quiz question is underlined.
1. If you divide the total recommended weekly minutes for moderate
physical activity, into equal weekday periods, that EXACT time period
would replace:
A. Breakfast at Brennan's
B. Licking and applying a Forever stamp
C. Mixing a chocolate cake batter
D. Running a 10K race
E. Watching an episode of "The Conners"
A Brennan's breakfast easily requires one hour. Putting a stamp on an envelope rarely takes longer than a minute. The preparation time for a chocolate cake batter? 20 minutes tops. A 10K race can be run in about 45 minutes by a top - tier runner. The allotted time for a comedy like "The Conners" is 30 minutes, and that is the daily average time a person might expend on moderate physical activity. Thanks to the American Heart Association, and Department of Health and Human Services, for this recommendation.
2. To protect your cells and keep your skin healthy, eat plenty of foods high in Vitamin C.
The Office of Dietary Supplements at the National Institute of Health provides a deep review of Vitamin C's powers. Try to consume the vitamin in uncooked foods, since Vitamin C is water-soluble. Cooking otherwise limits the effectiveness of the vitamin, so that you consume additional nutrients and fiber from uncooked foods, as well get increased nutrition. And, yes, getting at least your recommended daily allowance of Vitamin C can be a cardiovascular benefit.
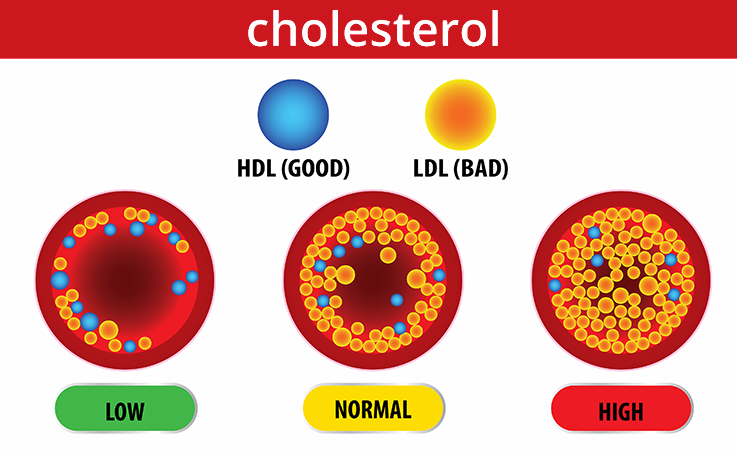
3. All cholesterol is bad for your heart and blood vessels. T F
The Centers for Disease Control and Prevention point to high - density lipoproteins (HDL), or "good" cholesterol, as a source for production of hormones and cell construction. Keep your HDL to LDL (low density, or "bad cholesterol") high, and manage your LDL through lifestyle changes and your healthcare provider's assistance.
4. Describe common behavioral methods for managing your triglyceride levels.
According to the Cleveland Clinic, you may have a significant chance to lower your triglyceride levels in your blood when you get regular aerobic exercise, eat healthy and maintain a weight that is good for you. For example, a diet that may be helpful in lowering triglycerides would include: low amounts of fats, of sugars, and of simple carbohydrates and alcohol. Your healthcare provider might direct you to consider medication (e.g. statins) to manage very high triglyceride levels.
5. Areas on your body that do not allow for reliable blood pressure readings include:
A. Earlobe
B. Finger
C. Toe
D. Upper arm
E. Wrist
The American Heart Association says that blood pressure cuffs, fitted around the upper arm, provide the most reliable blood pressure readings. Even though wrist cuffs are available in many 'big box' stores, their reliability is suspect. Earlobe and finger readings are not widely accessible outside research or clinical settings.
6. Supplements like ___B vitamins____ and __magnesium_____ help stabilize your blood sugar levels.
A 2015 paper in the journal Endocrine, Metabolic and Immune Disorders Drug Targets by Valdes'-Ramos et al., included the conclusions that eating foods containing ample amounts of the nutrients above, among others, is the best approach to increase control of type 2 diabetes. Use of dietary supplements to augment other medical treatments for diabetes, remains an individual decision until further research fills in the blanks about supplements' roles.
7. Reluctance to eat protein could be a sign of kidney disease. T F
A 2018 meta - analysis in PLoS One of 19 randomized controlled trials, on the relationship between protein consumption and chronic kidney disease (CKD), revealed that the rate of decline in kidney function, as well as the risk of kidney failure for persons with CKD, may be slowed by a low - protein diet. Not wanting to eat protein, by itself, indicates you may have kidney disease. There is still limited understanding of how much protein consumption among cohorts is best.
8. Explain how rheumatoid arthritis can lead to cardiovascular disease.
Inflammatory processes engaged in the body by rheumatoid arthritis (RA), can lead to buildup of lipoproteins that may bring about cardiovascular disease. Be proactive! Reduce your levels of inflammation. Treat signs of cardiovascular disease. Fight the risk factors hard!
9. Women's health risks that do not trend with cardiovascular disease include:
A. Hormone replacement therapy
B. Mommy's locked in the bathroom
C. Oral contraceptive use
D. Pre - eclampsia
E. Preterm delivery
Option "B" is a temporary respite from shocks to the heart.
10. South Asians will benefit from lower cardiovascular risk, by focusing on their best levels of _HbA1C_, _physical activity_ and _carbohydrates in the diet_ (Cardiology magazine, 5/17/2019).
11. E - cigarette use is safer for adults than smoking or otherwise using tobacco. T F
The U.S. Surgeon General, the Department of Health and Human Services, and Northwestern University Medicine each document on their websites, factors including the ingestion of toxic minerals (e.g. aluminum, tin, nickel), the consumption of high levels of nicotine relative to that in tobacco, and the potential for both injury to the developing brain, and the lungs, which point to e-cigarette use as extremely risky to health.
12. Talk about what habits of yours have most helped you maintain a healthy weight.
I keep a balance in my life, that helps me keep my weight where I need it to be. I watch the portion sizes of my meals, so I get the nutrition I need. My daily diet allows me opportunities for sufficient protein, fiber, essential nutrients and water. I exercise at the level that affords me at least moderate cardiovascular benefit. Stress I manage through my fitness work, cognitive - behavioral work, and leisure pursuits. I sleep to refresh the brain and body. It's a constant discipline, with pauses inserted to relax and 'cheat'.
13. Takeaways from any discussion of a genetic predisposition for CVD should mention:
A. If you have CVD, your siblings have a 40% greater risk of developing CVD.
B. You face a 60 - 75% higher risk of CVD, if your parents presented with CVD.
C. Nothing you might achieve from lifestyle management can lower your CVD risk.
D. Your risk for having a heart attack (myocardial infarction) is increased, if one parent had an MI.
E. The Developmental Origins of Health and Disease
framework gives researchers and clinicians, tools for better
understanding the transmission of CVD between branches of a family tree.
Two 2014 studies published in the journal Canadian Family Physician cite statistics for options "A", "B", and "D". A 2018 paper in the Journal of Physiology takes the study of pre- and perinatal effects upon the health of individuals to a mechanistic level,by comparing the fetal developments of humans with those of guinea pigs.
THERE. I hope you've enjoyed the brief experience in the wide world of cardiovascular disease. It's also my wish that you see there is a place for the SLP clinician, helping her consumers learn to manage risk factors for CVD.
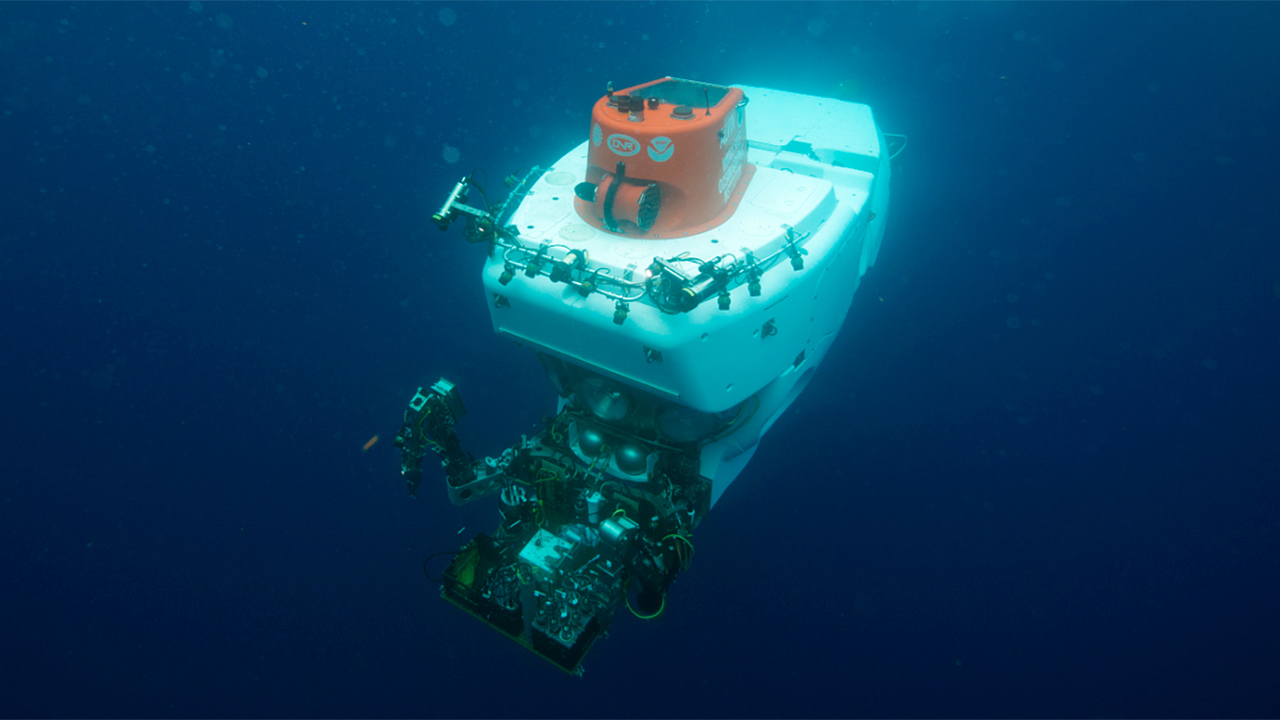
Loneliness. It seems to fit this profession, speech - language pathology. At its core, SLP requires one person to engage with one other person in an isolated space, a metaphorical 'diving bell', and then - the engagement is done. You meet and make a contract, outside of real life, with a person in need; you help that person improve the quality of her life; then the person returns to real life, while saying goodbye to the deep - diving SLP. When does the next dive commence? "Come dive with me", Sinatra might have sung. The SLP helps bring the consumer out of her loneliness, borne of an impairment. The SLP lives her loneliness, part of her mission.
Thanks to the artists cited below, whose thoughts on loneliness turn it about like a newly cut gem, with facets that reflect back the truths of the issue. Is there a popular, or even an obscure song about loneliness that you feel tells a lonely tale the best? If you are an SLP doing clinical work in one or more settings, does the notion of SLP being a lonely job, resonate with your experience? Let's explore further, after the musical interludes.
https://youtu.be/eFvenjll1Bk
https://youtu.be/65PcmJRfgl0
https://youtu.be/E3MNG11oynA
https://youtu.be/ojdbDYahiCQ
https://youtu.be/djU4Lq_5EaM
https://youtu.be/kjq4wYuwgxs
https://youtu.be/6EEW-9NDM5k
https://youtu.be/Tdw7kxD8eUc
https://youtu.be/RLM0tiZ5Kf8
https://youtu.be/FXmbIRUP7k8
After all, we are the experts in what we do. Everyone thinks they can do speech therapy, but we are here because we know why - why what we do works. We go to classes with peers and friends, and we socialize with peers, partners, and friends. Still, as our skill sets are nurtured and grow, we develop the power and the confidence to effectively work alone. Each new referral to an SLP takes us on a solo voyage, but the solo voyager is the person we serve.
It's as if we are invisible; that is, we are solely a conduit for the change that the consumer seeks. That might seem a totally magical, fantastic concept, but the more you work with consumers, the more you may notice that the consumer should get all the attention. As the aspiring SLP evolves from student, to clinical fellow and then to certified clinician, the clinician celebrates becoming an autonomous, solo professional who is happy to let her consumer be ' the star of the show.'
With all that has been said in this blog, about the power and value of the therapeutic alliance, - it is equally important that the alliance be ended as easily as it is initiated, firmly. The alliance is forged at the evaluation, and the SLP initiates the plan of care, by thinking about how it might end.
I found myself back in the position of Charlie Brown at Christmas, asking if anyone can tell me what SLP is all about! I realized that the loneliness I had been feeling, was in part missing myself; missing the fullest expression of who I am, and why I do what I do. I hadn't been able to put into words in a focused manner, what I have been attempting to do in the blog for almost ten years. Yet with staying peaceful, the thoughts and feelings about what the last 38 years have included, flowed. The words finally came:
* keeping communication natural is best, and especially in the clinical setting;
* making the deepest connection during the therapeutic alliance, is ideally attainable in 'real life'.
* what the consumer and her supports may want during the alliance, should drive the plan of care;
* though addressing changes in function at the impairment level is the bedrock of our skill sets, this aspect of clinical practice isolates the consumer and the SLP from what communication does - bring people together;
* SLP intervention not only puts the consumer 'up on the greaserack' to mediate the impairments, but also to take the consumer 'out for a spin', where real life exists for the consumer;
* The SLP that is embedded in real life serves a community, as well as those who consent to the therapeutic alliance;
* the community gains an advocate for staying well, through the SLP helping everyone limit or eliminate risk factors for impairment;
* SLP's are prepared for and invested in the power of the therapeutic alliance; it is our portal to what we do;
* a healthy therapeutic alliance will, nevertheless, end in most cases, leaving the CSD professional momentarily 'lonely'
* the SLP will be in the community and for it, and for the persons who discover their needs;
Like Raymond Chandler's perspective on the private detective, the SLP is a lonely person. That person will still celebrate her community. The community is much better for that.
"We've gotten a new swallowing order; I know it's almost the end of the day, but can you do it?"
"We hire speech therapists as PRN only; you get paid for patient contact - no benefits"
"We have three therapists on the case, so your involvement we staged to start last - and you have just 2 visits "
"Others, like OT - they can work on cognition"
"I need to continually educate the nurses and doctors, about what we do"
"Good communication is basic to how the healthcare team works best"
"People need to communicate and swallow continually; if you can't do direct service, do education and counseling until direct service can start; a flat fee can be charged for the service"
"You continually GIVE your time, above and beyond the patient contact time, to do all the work that need be done."
"There's no budget for equipment, materials, supplies; it's rewarding, regardless, to hear and see satisfaction on a consumer's or family's face, when you have given them something that helped"
"Training and experience are stern teachers; the SLP can function well within any worksite, contributing to team management of successful consumer outcomes, and the discipline and focus on function the field can bring".
We were blessed last year in the upper Midwest (USDA Hardiness Zone 5b), that the summer garden took off like a rocket. The occasional heavy rains needed supplementing a few days a week with my watering labors...a 2 gallon watering can does the trick, because even though more trips are required to give the plants a drink, there's exercise. Clover made its resurgence, after three years of being dormant. More than 95% of all the seed varieties that were sown, were germinating and thriving! I couldn't ask for more from the soil - it's black, moist, and with strata allowing for plentiful movement of root growth, and - after more than ten years of continual amendment, showing signs of proliferation of good organisms that feed the vegetables, flowers and herbs.
But - when all the produce is grown to its best, harvested and processed; what to do with it all! You gardeners who work so hard, year - round to keep the garden ecology viable and productive, how do you make the fruits of your garden work for the greater good? Those clinical programs in SLP that utilize a garden for training staff; - whether they be future clinicians, current staff or those community volunteers who would like to help - they might benefit from your skill set, and they might further the movement of their mission.
What I am saying, is that CSD training programs that support training gardens should develop, alone or in collaboration with other entities, tasting kitchens that serve consumers, their stakeholders and the community. A "tasting kitchen" will provide the practicing speech - language pathologist, who works with persons having swallowing problems, opportunities to directly train the consumer in the set of swallowing skills desired, with fresh food. The tasting kitchen will afford the SLP clinician to balance the needs of consumers to eat safely, against the need of consumers to eat well.
Of course, cooking and preparing foods for persons with swallowing needs is significantly outside the field's scope of practice. But there are obvious advantages to having this unique service offered to consumers:
* the consumer is reassured that her/his quality of life - in this case - the desires and needs for nutrition and hydration- may more easily be met.
* the SLP can liaison with professionals in many fields, who have an influence over what we can buy and eat: gardeners, farmers, grocery stores, chefs, nutritionists, dieticians, food anthropologists, cookbook writers and owners, and restaurants, diners and cafes: they can be the food professionals, providing the real material for direct dysphagia treatment;
* the 900 pound gorilla in the room (who the heck pays for this?) can be assuaged by a fee - for - service arrangement, or underwritten by grants, fundraisers and other external supports;
Let's contemplate how the SLP tasting kitchen might increase the odds, that our consumers might achieve the swallowing outcomes they desire.
I think occasionally, of the total number of persons I have served during my SLP career of....thirty-eight years this August. If you had lined up all my consumers over all the years, their standing in line six feet apart, I can imagine the queue would have extended from my home, to the farthest reaches of the galaxy. My practice often has been a far - flung galactic outpost, far from the prestigious healthcare institutions, the University training grounds and the well-funded school campuses. The opportunities that have come along, and the circumstances that have steered the work from job to job, from condition to malady, have steeled me to a realization about a speech-language pathologist:
an SLP is a taxi driver, taking the person served from a temporary to a transitory location. But I almost had a lapse of awareness, for the present day. You might also say, an SLP is a ride - share driver.
Get the call, pick up a fare, head straight for the destination wanted. In spite of the desire of the professions to make patient care in CSD "person - centered", or "personal", clinical work day - to - day is a series of pick up, travel, disembark; pick - up, travel, disembark. There is no inherent reason to act otherwise, though your job is to help your passenger grow more confident, more independent and more in control. We drivers for better communication and swallowing; we are to get our passengers from Point A to Point B in a timely fashion, and precisely finding the destination. The consumer wants it. The support circle is waiting. Those who pay the rider fare expect you to arrive on time. The managers of your business have more fares ready to pick up.
But the journey! Oh, the places you'll go! The courage to be found, and the sights to be seen....those moments of insight, of pain relieved and strength bolstered....the journey is the thing, and it is why you are hired. Your consumer, your passenger shows you the way to go. It's your expertise in piloting, that gets the passenger to the endpoint (s)he wants. The sights on the journey; they make it almost sad that the journey has to soon be over.
And it does have to end, and it does end. The alliance, the bind forged at the start of the galactic journey is dissolved. But another passenger, another consumer needs you now. The galaxy awaits.
Some months ago now, I was suddenly awash in the realization that I had accumulated nothing to leave to the world, before it was my time to leave it. While it's been a big part of my motivation for this blog, to leave a legacy of speech-language pathology as I see it: that's it the best kept secret in town; that it's a profession so poorly misunderstood, and because it's poorly represented in our culture; that it had allowed the hopelessly nerdy science geek with a deep love of the arts to meld together all his interests, and become a human service worker that affects a fundamental need of everyone: communication with our fellow human beings....I don't feel I've helped make a difference, yet.
What sometimes makes a life or career distinctive, is highlighting those points in time where decisions were made, actions taken, that altered the course of your day - to - day existence. Each of us can get caught galloping so hard inside the hamster wheel, no matter our life path, that it's hard to see the bigger picture - hard to get the perspective of experience and clinical judgement that helps you decide "What Does it All Mean?". The blog affords me that opportunity to "zoom out", and make sense of the many events that have made a difference in my life. Previous posts in this blog have already highlighted some of the important periods in this SLP odyssey:
November 9, 2012: "What I Want to Do"
You devote your time to doing things with words; to eating with pleasure anywhere you want.
November 28, 2012: "Primary Prevention Products"
You can obtain low-cost, real-world tools that help you stay fit for thinking, for talking and swallowing throughout your life span. .
September 22, 2013: "Information Has to Get In To Be Used"
You not only have difficulty understanding individual words, but you also lose the power of interaction when hearing loss becomes cognitive loss.
June 29, 2014: "Organic SLP"
Instead of carrying over the effects of impairment-based therapy to real life at the last visit, you focus on real - life function from the beginning.
February 29, 2016: "Wellness for your Career, for your Life"
You need to have a plan, or plans, to manage conditions for burnout, and keep your work and life balanced.
July 3, 2016: "Pneumonia and Its Discontents"
Confront your mentor; if that person has lost the luster that you had applied to her/him, in the formative years of your career, there's still hope.
November 4, 2016: "My Ethnography"
Know the culture of your consumers and stakeholders; know the culture of the therapeutic alliance.
November 26, 2016: "Why Ethnography?"
Your successful outcome is helped by maneuvering the cultures in which the consumers and stakeholders exist;
July 9, 2017: "Cherry Cherry"
Gather ye evidence while ye scour/all the best sources, no matter the hour.
April 23, 2017: "Communication Fitness"
You can do some simple things, some of them perhaps in unusual contexts, to sustain or improve your skills, throughout your lifetime, BEFORE therapy is called for.
January 1, 2018: "Be An Entrepreneur "
You should sell what you do; provide superior customer service, and your business acumen will be known by more and more people.
January 3, 2019: "On the Other Side"
When you're a caregiver, you understand caregivers better. You can help empower them, so your consumers can do better.
January 27, 2020: "Goodbye, Dr. Carey"
Who am I, as healthcare becomes most visibly a business...? Not a stable pony; not interchangeable. The SLP must function as part of a system, and be respected for the quality brought to the system.
January 4, 2021: "Swallowing at the Crossroads"
Swallowing rehabilitation is influenced by layers of scientific, social, technological, political and moral forces. So are all the other interventions you might provide to consumers.
This is a list of some of my professional pivot points, or times in my life where I said 'aha' and my world made more sense. What are yours?
This blog has begun to plumb your depth of knowledge, about modes of intervention to prevent cardiovascular disease (CVD). Is there a possibility prevention activities could become a significant product line for most speech - language pathologists (SLP's)? Another way to ask the same thing: can SLP's serve their communities above and beyond their traditional roles as clinical practitioners, through education and advocacy, so that risk management for conditions e.g. CVD is proactive, focused and accessible to all?
CVD remains the top cause of mortality in the United States, according to the 2018 National Center for Health Statistics publication, Mortality in the United States. Stroke and other cerebrovascular diseases ranked fifth among the leading causes of death. In addition, the National Institute on Deafness and Other Communication Disorders reports that 1 out of every 250 persons suffers from aphasia, an impairment in the use of language because of cerebrovascular insult. SLP's, specialists in the diagnosis and management of cognition - communication impairments, have a mandate to include prevention activities in their scope of practice.
What follows is an example of a prevention tool that an SLP clinician might utilize with adult consumers of prevention services: a CVD prevention TRIVIA GAME. The game questions selected encompass selected knowledge domains, from the 2019 American College of Cardiology/American Heart Association Guideline on the Primary Prevention of Cardiovascular Disease. Those domains include physical activity (here called FITNESS), nutrition, obesity (called here WEIGHT CONTROL), diabetes (BLOOD SUGAR), lipids, hypertension (BLOOD PRESSURE), and tobacco (SMOKING).
Risk - enhancing factors, identified in the 2019 joint guideline, were also utilized to select game questions. They encompass family history, kidney function, inflammatory conditions, gynecologic risk and ethnic risk factors. Additional domains, described as social determinants of health by the Office of Disease Prevention and Health Promotion, Department of Health and Human Services, will yield game questions in the areas of economic stability, education, social and community context, health and healthcare, and neighborhood and built environment.
Your feedback is not only welcomed, but sorely needed. Thanks for your interest in growing the field. Stay safe!
CARDIOVASCULAR DISEASE PREVENTION TRIVIA:
Select the best answer for each question below, unless specific directions direct a different response.
1. If you divide the total recommended weekly minutes for moderate physical activity, into equal weekday periods, that EXACT time period would replace:
A. Breakfast at Brennan's
B. Licking and applying a Forever stamp
C. Mixing a chocolate cake batter
D. Running a 10K race
E. Watching an episode of "The Conners"
2. To protect your cells and keep your skin healthy, eat plenty of foods high in Vitamin ________.
3. All cholesterol is bad for your heart and blood vessels. T F
4. Describe common behavioral methods for managing your triglyceride levels.
5. Areas on your body that do not allow for reliable blood pressure readings include:
A. Earlobe
B. Finger
C. Toe
D. Upper arm
E. Wrist
6. Supplements like _______ and _______ help stabilize your blood sugar levels.
7. Reluctance to eat protein could be a sign of kidney disease. T F
8. Explain how rheumatoid arthritis can lead to cardiovascular disease.
9. Women's health risks that do not trend with cardiovascular disease include:
A. Hormone replacement therapy
B. Mommy's locked in the bathroom
C. Oral contraceptive use
D. Pre - eclampsia
E. Preterm delivery
10. South Asians will benefit from lower cardiovascular risk, by focusing on their best levels of _______, _______ and _______.
11. E - cigarette use is safer for adults than smoking or otherwise using tobacco. T F
12. Talk about what habits of yours have most helped you maintain a healthy weight.
13. Takeaways from any discussion of a genetic predisposition for CVD should mention:
A. If you have CVD, your siblings have a 40% greater risk of developing CVD.
B. You face a 60 - 75% higher risk of CVD, if your parents presented with CVD.
C. Nothing you might achieve from lifestyle management can lower your CVD risk.
D. Your risk for having a heart attack (myocardial infarction) is increased, if one parent had an MI.
E. The Developmental Origins of Health and Disease framework gives researchers and clinicians, tools for better understanding the transmission of CVD between branches of a family tree.
Speech - language pathologists (SLP's) are being engulfed in an identity crisis, within the community of healthcare providers. Among primary care physicians, medical speech-language pathology services are often an afterthought. Given the history of confusion over the name of its practitioners, it is confusing to their stakeholders that SLP's in healthcare now get the majority of their work from swallowing referrals. There are also concerns about the burnout rate among SLP's; the relatively flat salary schedule for healthcare clinicians; requirements by employers that their clinicians are ALWAYS available; the need to justify your existence with continually high productivity; - but there is also hope for the healthcare SLP who feels she/he is being compartmentalized as a "swallowing technician".... I actually was called that once by an internal medicine resident....mortifying, to say the least, when medical SLP's have to know how swallowing works in its complexity, and we must know how to work with people who need swallowing help. Doctors. What a mess they can make.
The medical SLP who dives into each day of swallowing problems, will swim toward an intersection of known scientific - cultural - political phenomena, that will be significantly addressed by the involvement of SLP clinicians. Sea changes in social science, in health, in politics and in culture will also serve the personal and professional growth of SLP practitioners, as we confront their effects on the field. Let's briefly identify a few of the intersecting forces, with potential to affect clinical practice patterns.
1. Dysphagia management: there is a realization that, even though the
technology exists to provide modified diets, safe to swallow by persons
with diagnosed dysphagia - the consumer may not want to eat the diet! Practice trends exist that allow the consumer and her supports
to train for swallowing a 'normal' diet, through use of compensatory
strategies. With this approach, a modified diet should be considered a
temporary intervention in the majority of dysphagia management cases. "I
can eat my favorite food, when I ____", is the outcome desired, not "I
can eat my favorite food, when it is prepared by ____". When you can offer your consumer potential to consume their preferred diet, they will often work hard for you - for THEIR goals.
2. Food viscosity: When you change the viscosity of a material, you
affect its ability to flow through a conduit. A consumer of SLP
services, who wishes to improve her swallowing of favorite foods,
will have viscosity as one powerful tool. Can you chew and manipulate a
pretzel bun to the consistency of oatmeal, through your mouth to TRIGGER
the swallow in your throat? Do you swallow the ginger ale right out of
the bottle, or does it need more mass to be easily felt and controlled
past your airway? Dedicated viscosity modifications, the product of
modern science, are easier than ever to find in pharmacies and big box
stores. Can any more natural change agents do the same? Clinical
experience says YES. Talk with your clinician for details. When you can augment the foods your consumer likes, so she can eat/drink them, they will often try their best.
3. Cooking: making not only the food easy to swallow for persons with dysphagia, but also tasty, convenient and palatable, is the mission of the family, the cooks, the servers, and the activated patient who prepares the consumer's diet. Is it served as it was intended, or is it cold? Will flavors and seasonings enhance the taste, and the enjoyment of the food and drink? Are salt, fat, acid and heat appropriately utilized to make this, the best meal your consumer has had recently? Does the place where the consumer is eating, help focusing on swallowing better? Are drinking vessels, utensils, condiments easily used? If an SLP and the consumer's supports can tailor the meal to the consumer's changing needs, then you might have the therapeutic alliance you want. The patient can eat for pleasure, while consuming an appropriately safe diet.
4. Urban farming/community gardening: giving the SLP consumer food and
drink she/he wants to eat, might include making available locally grown,
fresh and nutritionally dense food. Both urban farms and community
gardens can provide seasonal fruits and vegetables, which when grown
organically and harvested timely, can heighten the experience of eating a least restrictive diet. A consumer that enjoys easily eaten food, grown
cleanly and locally, may even want to grow some of her/his own food. When a consumer and her supports gets involved in bringing the food to their table, savoring it can make it easier to swallow.
5. Locavore: the person who eats like a locavore, regards the food grown locally and available only in season.
There may not be an immediate connection between an SLP consumer's dietary plan, and the decision to eat only locally produced food. Yet the consumer who consumes only locally grown food, helps change dependence of a food community on a global food supply chain. When you want to have a supply of a seasonal food throughout the year, you rely on traditional food preservation methods, eg canning or drying, to keep available longer, the food you want to eat. A local food consumer has a closer connection to the environments where food is grown, and where it is consumed. When you can eat seasonally, locally, cleanly, you have the best of all possible foods.
6. Culinary medicine: Approximately thirty clinical training programs
around the world help physicians learn to properly prescribe food as a
treatment for medical problems. Liaisons with nutritionists, chefs,
dieticians, food scientists, food industry representatives, consumer
groups and others may aid your family doctor, to guide you to the best
dietary solutions for your health. Will your doctor give you samples (amuse bouche) in
the office? Does the industrial food industry throw lots of money at physicians, with the goal of delivering cheap, mass marketed and convenient-to-produce food, to consumers?? When your primary care physician has access to food as medicine, you have available a medicine with centuries of proven effectiveness.
7. Food insecurity: Communities of all cultural, ethnic and economic stripes do not have adequate access to healthy food for many of its citizens. The roots of food insecurity may lie partially with limited personal income, with limited public support for food support programs and limited perspectives by the public, about the persons seeking food security assistance. Helping our food - insecure families, neighbors and communities get those resources to feed themselves, can be a rising tide that raises all boats. Food insecurity, hunger, poverty, chronic disease, economic stagnation, educational ceilings, and political instability: each are a pressure wave pushing against the stability of the culture. When food markets find their way into "insecure" neighborhoods, so that people of all levels of society have equal access to good food, we have a healthier society.
8. Environmental justice: a community resident inhales polluted air, or ingests food or drink contaminated with toxic material that endangers generations of residents. The toxic material often has an industrial source, placed in close proximity to residential areas when residents had little political power to keep the industry out. Industrial byproducts e.g. coal ash, heavy metals, and corrosive solvents accumulate in the industrial site - challenging the quality of life frmor residential sites. Industries have little incentive to clean up their byproducts, for civic leaders do not wish to alienate the generators of tax revenue and payroll for their jurisdictions. The cumulative effects of exposure to toxins for community residents, will often lead to chronic disease, if not severe afflictions that are atypical for the disease prevalence.
9. Climate change: It is a long - kindling inferno. No matter its presentation, the warming of our climates degrades our ability to grow food. Limits on water access yields limited ability to raise plants and livestock. The ecology that supports food production loses its equilibrium. Limited food production opens a Pandora's Box of stress on food and financial markets. Societies having difficulty feeding themselves will fight to control resources. When persons can't find food for themselves and their families, they will do what is necessary to survive. As data from NOAA illustrates, average annual world temperature has grown logarithmically since 1980. How much more time do we need to achieve climate justice?
10. Forest bathing: in Japan, where the practice originated, it's called 'shinrin-yoku'. A forest bather spends time in nature for refocusing, reflection and healing. Turn off and set aside your technology, when you forest bathe. You ultimately discover that the experience can be created, out of the forest. It's possible, even in your garden.
11. DoHD: The Developmental Origins of Health and Disease hypothesis suggests that critical periods, cumulative disadvantage, chains of risk and accumulation of social determinants can constitute an approach to effective management of health risk through the life span.
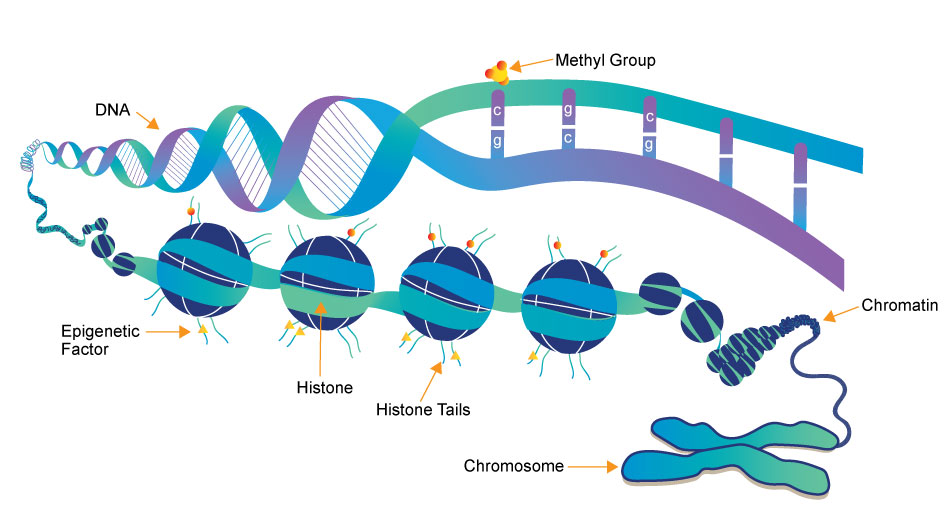
12. Epigenetics: social and environmental influences on health have been reflected as changes in the structure of chromosomes. Not only will your grandparents' behaviors have influenced your own health, but your health status will be reflected in the genetic potential of your descendants.
13. Life Participation Approach: in spite of significant impairments to function, including breakdowns of independent feeding and swallowing, consumers of SLP services can be helped to eat some of the foods they want. Making it possible to safely/efficiently swallow foods, might keep the consumer participating in the social network.
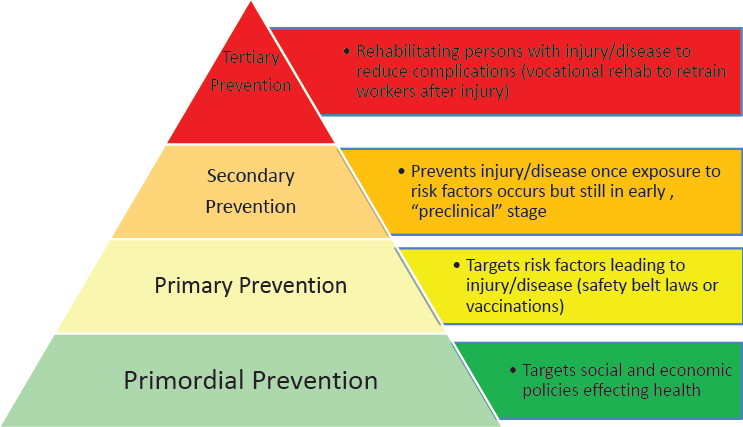
14. Primary vs. Primordial prevention: SLP clinicians who have become accustomed to prevention at the secondary level (identifying persons with impairments), will now find prevention can occur at primordial (prevention of risk factors for disease) or primary (modification of the risk factors) levels. If the SLP clinician wants to augment a clinical practice with prevention activities, e.g. assisting a consumer in improving the quality of food eaten, that clinician has a larger world in which to work. The big world will be much more conscious of what SLP does.
Happy New Year, blog readers! We are all ready for a fresh start in 2021, and this posting reflects my need to start towards a new horizon for my CSD work.
You'll find below a link to a second survey, that wants to find out how much you know about cardiovascular disease (CVD), what causes it, and how its impact can include the onset of speech, language, cognitive and swallowing disorders. I hope you find the survey interesting, and that it might whet your appetite to learn more about CVD, and how prevention efforts against it must start as early as possible for your consumers.
You'll find the survey at https://www.surveymonkey.com/r/TFT87DH
I hope you might complete the survey by 1/31/21. Thanks for your interest.